Infectious Disease: Physician Information
Evolution of the Technology and the History of SPAR
In December, 1990, the First International Symposium on AIDS and Reproduction was convened in Genoa, Italy. Dr. Kiessling was invited faculty because her lab was the first to measure HIV in semen in 1983-84 (Borzy Ms, Kiessling AA. First International Conference on Acquired Immunodeficiency Syndrom (AIDS), Atlanta, GA, 1985), and because of her Letter to the Editor in 1989: “Retroviruses and Reproduction,” Fertility and Sterility, 51: 756-758” The title of her talk at the Genoa Symposium was: The Role of Assisted Reproductive Technologies in Yielding HIV-Free Offspring of HIV-Infected Parents. In: Mellica F, ed. AIDS and Human Reproduction, S. Karger AG, Basel Switzerland. 1992:139-144.
Dr. Augusto Semprini, the founder of the “sperm washing/IUI” program in Milan, Italy, attended the congress. During the course of the congress, Drs. Semprini and Kiessling met to discuss the options for helping HIV infected men with uninfected female partners parent. He was faced with the reproductive needs of Roman Catholic IV drug abusers in Milano whose female partners were not HIV infected.
Dr. Kiessling’s concerns at that time, and to the present, include the fact that HIV is present in semen in two forms: free virus particles and infected leukocytes. Free virus particles may be infectious, but they are more fragile than infected cells and may be “washed” away from the sperm. Although there are several laboratory methods for separating leukocytes from sperm which take advantage of differences in size, density and sperm motility, it is still possible that “washed sperm” could be contaminated with infected leukocytes which are not detected. The most sensitive style of counting chamber is the hemacytometer used to count blood cells; the limit of sensitivity is one leukocyte per grid counted which is equivalent to approximately 10,000 cells per cc of semen. Therefore, 9,999 leukocytes per cc of semen or “washed” sperm would not be detected in this chamber. The chambers used by computer-assisted microscopy are less sensitive, (e.g. the Makkler Chamber). One leukocyte in a Makkler Chamber is equivalent to approximately 100,000 leukocytes per cc of semen. Therefore, 99,999 leukocytes per cc of semen (or “washed” sperm) would not be detected in the Makkler chamber.
Dr. Semprini decided to combine “sperm washing” with IUI for his HIV-discordant couple program in Milano. Dr. Kiessling decided to develop more reliable tests for HIV in semen before developing the guidelines for a program.
The Kiessling lab had measured viral burdens on the order of one hundred thousand to ten million virus particles per ml of seminal plasma from the gay men with AIDS in 1983-84. More recent molecular biology assays have confirmed those original estimates and revealed that antiretroviral therapy reduces, but does not necessarily eliminate, free virus from seminal plasma. Nonetheless, since a normal semen specimen contains on the order of one hundred million sperm, there are usually substantially more sperm in a semen specimen than free virus. It isn’t clear what percentage of virus adheres to sperm, but some elegant experiments from Virginia Scoffield’s UCLA laboratory in the early 1990’s revealed that the method of “sperm washing” greatly influenced adsorption of virus to sperm.
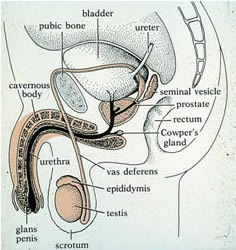
As is well-known in the assisted reproduction community, the biology of semen is complicated and not fully understood. Semen is a complex mixture of fluids and cells produced at ejaculation by organs, glands and tissues of the male reproductive tract (testis, epididymis, vas deferens, seminal vesicles, prostate and urethra). Sperm, on the order of 100 million per ejaculated specimen, are contributed by the testis, epididymis and vas deferens. Sperm mature and become motile following several weeks of development in the testis and epididymis. Some immature spermatocytes which arrest part-way through development may also be ejaculated and are referred to as “non-sperm cells.”
Seminal fluid and other cells are contributed by the seminal vesicles, prostate and urethra. All semen specimens contain leukocytes, but the number varies widely from specimen to specimen and they may arise from any of the semen producing organs. Semen leukocytes, on the order of 100,000 to 10,000,000 per specimen are also referred to as “non-sperm cells.” Some immature sperm look very similar to lymphocytes and differentiating the two cell types requires immunostaining techniques.
The source of HIV infection in semen, either free virus or virus infected cells, remains unknown, despite many years of research in this area. What has become clear in recent years is that the burden of virus and infected cells varies widely from one specimen to the next and that the free virus particles present in semen are produced by a source of infection separate from the one that produces the infected cells. Therefore, more than one male reproductive tract organ is involved in the production of infected semen.
For these reasons, it became clear that the safest method of assisted reproduction to help uninfected partners of HIV infected men conceive was to use sperm from semen specimens with an undetectable burden of virus in IVF procedures. Therefore, methods were devised to fractionate semen specimens into aliquots for molecular biology assays of HIV RNA and proviral DNA, as well as leukocyte counts by immunostaining, and cryopreservation of the sperm. Sperm only from specimens with an undetectable burden of virus would be used for conception.
There were two ways to fertilize the eggs in the laboratory: either by exposure to 2 million sperm for one to two hours, or by injecting one selected sperm directly into an egg (intracytoplasmic sperm injection, ICSI). Moreover, because sperm can be cryopreserved (frozen to stay alive) for long periods of time, it would be possible for couples to receive care by fertility clinics close to their homes because frozen sperm from tested semen specimens could be shipped to those clinics. By shipping only sperm from specimens with an undetectable burden of virus, exposure of laboratory personnel, medical staff and other patients would be greatly reduced.
Therefore, the Special Program of Assisted Reproduction (SPAR) was designed with the following goals:
To add to these considerations in designing the Special Program of Assisted Reproduction, in 1991, the Centers for Disease Control and Prevention in Atlanta published the opinion that intrauterine insemination with “washed” sperm from HIV infected men had not been proven to be safe.
- An overall assessment of the health of the male and his antiretroviral regimen.
- The development of a sensitive, reliable procedure for testing semen specimens for HIV particles and HIV-infected cells
- The establishment of a program of In Vitro Fertilization for couples with infectious disease infertility in order to test the hypothesis that uninfected partners of HIV infected men could achieve a pregnancy without themselves or the baby becoming infected
- The development of methods for shipping semen specimens to the testing laboratory for sperm cryopreservation so couples could be cared for by infertility clinics close to their homes
Importantly, many of the HIV infected men seeking fertility treatment have needed referrals to HIV specialists, either because they were not on therapy or their therapy needed modification. The vast majority of HIV infected men seeking to parent feel the need to keep their HIV status a total secret. This frequently impacts their treatment decisions.
As of the end of May, 2011, 150 SPAR babies in total have born, all Moms and babies have tested negative for HIV infection.
In 2002, an adjunct SPAR program (oligospermia cup insemination) was designed to take advantage of the semen testing protocols and allow women to attempt to achieve a pregnancy without going through IVF or IUI.
In 1999, the first SPAR baby was born following IVF treatment in Boston. In 2000, the first SPAR baby was born following IVF treatment in a collaborating clinic in Arizona with frozen, tested sperm shipped from Boston.
A method developed many years ago uses a device termed an “oligospermia cup”. It is similar to a cervical cap and is designed to concentrate sperm at the opening to the cervix to allow them to swim through the cervix and into the uterus, as in natural intercourse. Comparisons of the pregnancy rates with IUI versus cup insemination reveal the methods are comparable with normal sperm counts, although IUI rates are higher with low sperm counts.
All women are tested for HIV antibody at 3 weeks, 3 months and 6 months following either embryo transfer or cup insemination. To date, all tests for all women have been negative.
For the adjunct SPAR program, the same semen testing procedures are used, but the frozen sperm from specimens with an undetectable viral burden are thawed and placed in the cervical cup for a period of 3 hours. The woman takes one dose of AZT just prior to the cervical cup procedure. At the end of 3 hours, the cup is removed. Two SPAR babies have been born from this procedure as of July 1, 2003, with one ongoing pregnancy.
We believe these data provide strong support for the position that HIV infection in males should be regarded as another form of treatable, male factor infertility. All that is required is semen testing for HIV burden and sperm cryopreservation.